Homeostasis is a tendency of interdependent elements to attain a state of constant equilibrium. Balance is the key to maintaining healthy bodily functions. Core temperature, blood glucose, sodium and chloride levels, body pH are a few systems the living body aims to take care of constantly.
The difference between acidity and alkalinity of the body is known as pH (potential of Hydrogen). It is calculated on a scale of 0-14, with 0 being most acidic and 14 most alkaline. Our body, functions to its optimal capacity at a pH of 7.3-7.45. This pH is essential for cells to perform their activities efficiently. Any upward or downward deviation in pH value can put the body in a state of excess alkalinity or acidity. Proteins may lose their original structure (denaturation), enzymes will not function properly and even death may occur in a few cases. Diseases mostly find their home in an acidic environment, which is why it becomes all the more important to take care of our health.
ACID-BASE REGULATION:
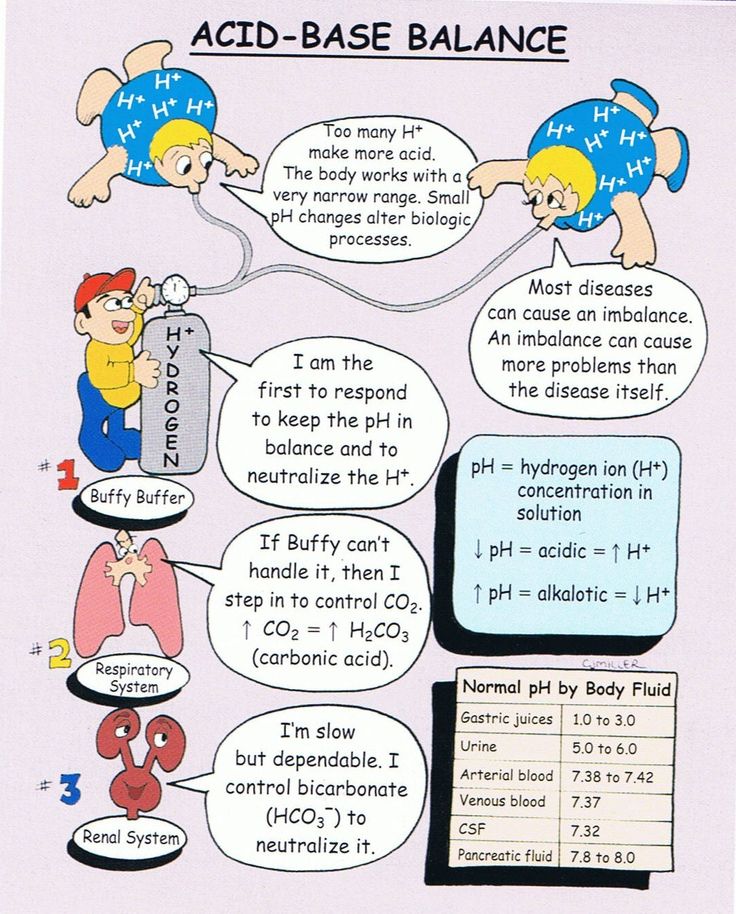
The acid-base regulation in the body is regulated by an interplay of the following mechanisms :
Buffering agents –
These are of two types, namely extracellular (bicarbonate, ammonia) & intracellular (proteins, phosphate). The bicarbonate buffer is of prime importance, since it can reversibly form carbonic acid and control the retention or release of carbon dioxide into the system.
Following the isohydric principle, where all acid-base systems stay in equilibrium with one another, homeostasis is achieved.
The respiratory system –
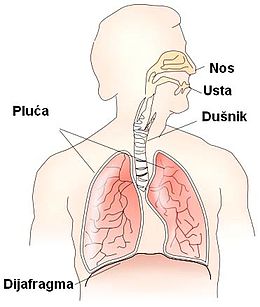
The prime function of our lungs is to inhale oxygen and give out carbon dioxide as a waste product. Carbon dioxide (acidic), excreted via blood, reversibly forms carbonic acid by combining with H+ ions. The blood reaches the alveoli of lungs, where carbonic acid again breaks up, or dissociates into carbon dioxide and water where CO2 is excreted via the airway by exhaling. The respiration center, located in the brain is responsible for regulation of respiration. So, any abnormality detected in the acidic (CO2) levels of blood will trigger the respiration center to increase or decrease the rate of breathing to control the amount of CO2 given out. By the excretion of about 12,000-15,000 mmols/day, this system has an efficiency of 50-75%.
The renal system –
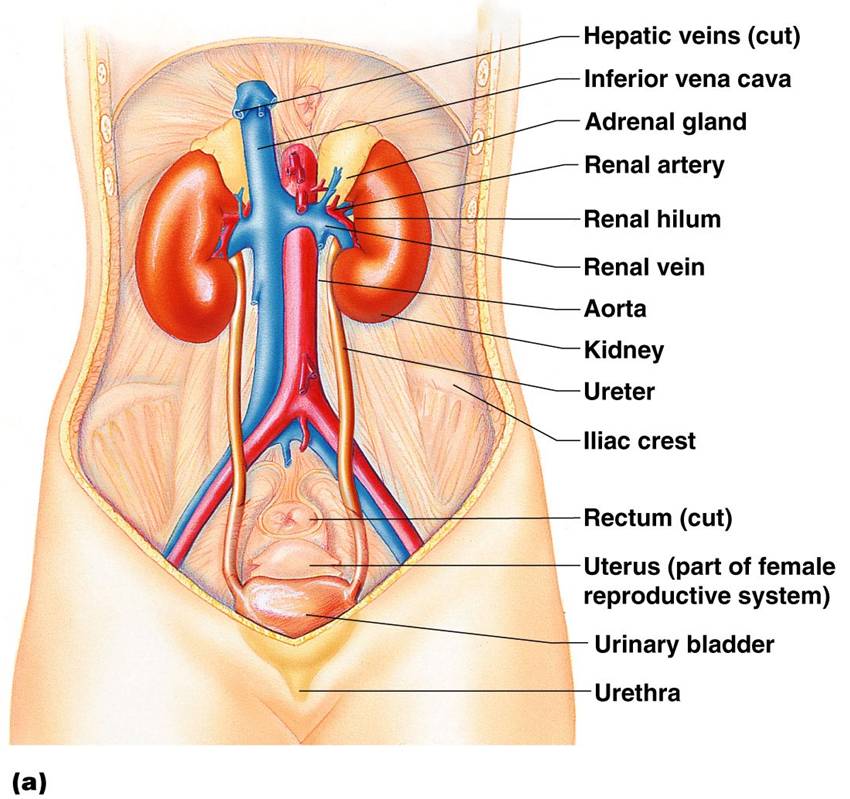
Where the lungs excrete carbon dioxide, the kidneys are responsible for elimination of ‘fixed’ or ‘metabolic’ acids. About 70-100 mmols/day are excreted by the kidney. The reason why it is very less as compared to the lungs is because this is the only exclusive pathway involved for fixed acids. Moreover, this amount is large compared to the plasma concentration of H+ ions.
Along with this, the kidney is responsible for reabsorption of bicarbonate which is filtered (approx. 4000-5000 mmol/day) which helps in maintaining the body pH.
In simple terms we can say that the kidney maintains the acid base balance via two mechanisms :
-
Proximal tubular mechanism –
Here, the bicarbonate ions are reabsorbed which were filtered by the glomerulus and in the second part ammonia is produced.
-
Distal tubular mechanism –
With the help of this mechanism, about 70 mmols/day of fixed acid is excreted daily. A maximum of 700 mmols/day excretion is possible too, but this takes about 5 days. Distal tubular section is responsible contributing to titratable acidity (amount of acid in a solution) of urine, addition of ammonium (NH3+) ions and reabsorption of the remaining bicarbonate ions.
What is Acidosis?

Acidosis can be defined as an excessive acid condition of the body fluids or tissues when the arterial pH falls below 7.35. This can be brought about either by acid accumulation or loss of alkali. Acidemia is a state of low blood pH, whereas acidosis is the process which causes acidemia.
This can lead to irreversible cell damage in extreme cases and affect the associated organs by extension, bringing about a range of signs and symptoms.
Now that we have understood the basics of acid-base regulation in our body, there are two chief pathways through which acidemia happens.
-
Excessive accumulation of carbon dioxide in the blood
-
Inability of the kidney to excrete ‘fixed acids’ out of the body, or the production of extra acid in the body, such as lactic acid
Classification:
According to the cause, acidosis can be classified into –
-
Respiratory acidosis
-
Metabolic acidosis
What are the sources of acid in the body?
Most of the acid in our body comes from :
-
Processing (metabolism) of carbohydrates and fats – The end result of metabolism of carbs and fats produces energy, water and some amount of carbon dioxide. Carbon dioxide is also a product of respiration. In the presence of enzyme carbonic anhydrase, this CO2 combines with water to form carbonic acid (H2CO3) and later on dissociates to give hydrogen ion (H+) and bicarbonate (HCO3-). The H+ produced will bind itself to red blood cells (RBC), travel to lung alveoli and again in the presence of carbonic anhydrase, will convert to carbon dioxide gas to be excreted from the lungs.
-
Lactic acids and ketoacids which are produced as a result of incomplete metabolism (in absence of oxygen)
-
Breakdown of phosphates in the diet in the presence of water (hydrolysis)
-
Sulfuric acid, which is produced after metabolism of sulphur containing acids (cysteine, methionine)
-
Metabolism of cationic amino acids (arginine, lysine)
What is respiratory acidosis? How does it happen?
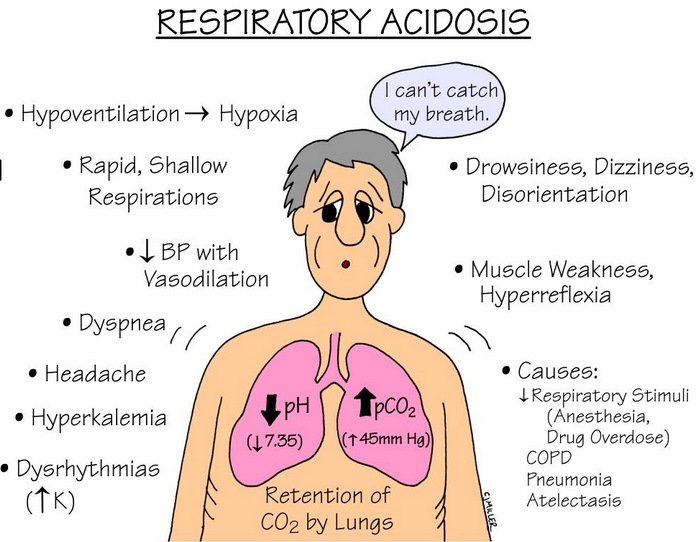
Respiratory acidosis will happen if the lungs are unable to expel carbon dioxide from the body properly. This will cause a buildup of carbon dioxide in the blood, a condition known as hypercapnia.
Respiratory acidosis is caused by –
-
Any condition hampering the lung function – Obstructive lung disorders such as emphysema (damage to lung alveoli), chronic bronchitis (inflammation of bronchi), pneumothorax (abnormal collection of air in lung space causing lung collapse), asthma and severe pneumonia.
-
Breathing disorders in sleep such as sleep apnea
-
Depression of respiratory centre due to head injury
-
As a compensatory response to increased alkali levels in the body
-
Overdose of drugs such as opioids and sedatives
-
Disorders of nerves and muscles which can result in chest compression and impaired breathing, as amyotrophic lateral sclerosis
-
Pulmonary edema
-
Scoliosis
How to tell someone has respiratory acidosis?
The presenting features of respiratory acidosis are a window to its cause. Some of its signs and symptoms are:
-
Headache
-
Drowsiness
-
Memory loss
-
Sleepiness
-
Coma
-
Hyperinflation, wheezing sounds
-
Cyanosis (bluish discoloration of skin and mucous membranes)
-
Clubbing of fingers (due to hypoxemia)
Metabolic acidosis:
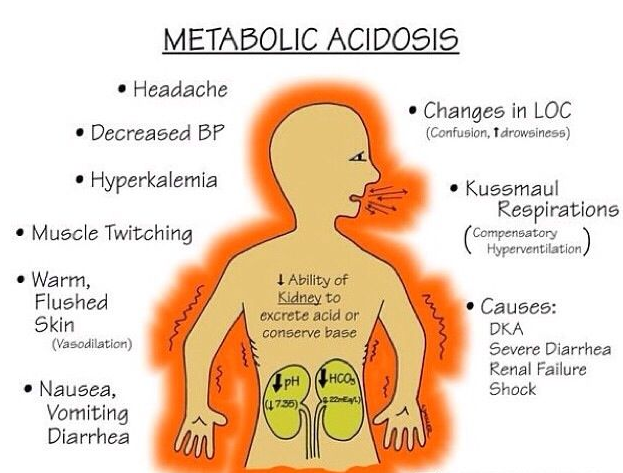
When there is a reduction in the amount of bicarbonate (HCO3-) in the blood due to production of excessive acid or when the kidneys are unable to filter out the ‘fixed’ acids, acidemia occurs and this condition is termed as metabolic acidosis.
Before we take a look at the causes of metabolic acidosis, we need to understand the ‘anion gap.’
ANION GAP:
Our body is composed of many electrolytes which can be divided into anions and cations. To maintain equilibrium (0 electric charge), the number of anions and cations should be equal. The difference in the levels of cations (Na+, K+) and anions (Cl-, HCO3-) in serum, plasma or urine is known as the anion gap.
The gap is determined not by a specific diagnostic test, but by a mathematical formula that uses the results derived from other tests (which tell the concentration of a particular ion in the body).
=( [Na+] + [K+]) – ([Cl-] + [HCO3-]) = 20 mEq/L
The common ranges that are used as reference are 8-16 mEq/L and 10-20 mEq/L. These values are based on the exclusion and inclusion of potassium ion concentrations. On the basis of these values, anion gap can be classified into high, normal or low.
Anion gaps help us to determine whether the acidosis is a result of imbalance in the electrolytes or if there is any other underlying condition.
The causes of metabolic acidosis are as follows:
High anion gap causes – (>12mEq/L)
-
Ketoacidosis – Accumulation of ketone bodies (acidic) in the body. Reasons can be diabetes, fasting, under nutrition and chronic alcoholism.
-
Lactic acidosis – Certain physiological processes can trigger this condition such as shock, seizures and decreased oxygen in the blood (hypoxia).
-
Lactic acidosis due to toxins – Poisoning due to carbon monoxide, cyanide, isoniazid, toluene, propofol, etc.
-
Kidney failure
-
Toxins converted to acids in the body – Methanol, salicylates, ethylene glycol
-
Short bowel syndrome, bacterial overgrowth
Normal anion gap causes (6-12 mEq/L) – Also known as hypochloremic acidosis
-
Bicarbonate loss from the gastro-intestinal tract – diarrhea, colostomy, enteric fistulas, use of ion-exchange resins, excess of Calcium chloride intake, etc.
-
Urologic procedures – ureteroileal conduit, ureterosigmoidostomy
-
Bicarbonate loss from kidneys – hyperparathyroidism, renal tubular acidosis, acetazolamide
-
Parenteral infusions – arginine, rapid sodium chloride infusions, lysine
-
Other causes – hypoaldosteronism, hyperkalemia
Signs and Symptoms :
Like respiratory acidosis, the metabolic variant’s presentation is a reflection of its underlying cause.
-
Chest pain
-
Palpitations
-
Headache
-
Deep, rapid breathing – Kussmaul respiration, associated with diabetic ketoacidosis
-
Nausea, vomiting
-
Loss of appetite
-
Weight gain
-
Muscle weakness
Diagnosis of acidosis :
Whether acidosis is a result of a ventilation problem or because of some serious deviation in metabolism, a diagnostic test tells you all. As soon as the cause is determined, immediate action can be taken to prevent this stage from becoming irreversible.
The approaches taken are :
-
Physical examination –
Here your doctor will evaluate the presenting signs and symptoms of the disease and try to form a provisional diagnosis. For e.g. Kussmaul’s breath indicates the presence of diabetic ketoacidosis, wheezing sounds may indicate a chronic obstructive respiratory disorder and indicate respiratory acidosis.
-
Blood gases –
Arterial Blood Gas (ABG) is a compulsory diagnostic aid employed to determine the pH levels of blood, its oxygen and carbon dioxide concentrations from an artery. It is an indicator of how well the lungs are functioning. A low serum bicarbonate and pH less than 7.4 indicate metabolic acidosis.
-
Electrolytes –
Here, the total electrolytes, including the measurable and unmeasurable ones such as Na+, K+, HCO3-, Cl- are calculated (anion gap) from different sources and the results are compared on an electrolyte panel to help determine the cause behind the disease. E.g. a high anion gap may point towards diabetic or lactic acidosis, whereas a normal anion gap may show hyperchloremic acidosis.
A nonspecific test, but elevated WBC levels may show the presence of an infection (septicemia), which can cause lactic acidosis. Less oxygen delivery due to severe anemia can cause lactic acidosis too.
-
Urinalysis –
Urine samples are analysed and examined for presence of glucose, ketone bodies, proteins (albumin). If the cause of acidosis is ethylene glycol poisoning, the analysis will reveal calcium oxalate crystals in the sample.
-
Anion Gap –
As explained earlier, the degree of anion gap can lead the doctor to perform specific investigations to find out the exact cause. A high anion gap is seen in diabetic ketoacidosis, lactic acidosis whereas a normal anion gap acidosis can be caused by diarrhea.
Urine anion gap is also calculated separately to rule out any defects of the kidney.
- Ketone bodies –
Acetoacetate, acetone and beta-hydroxybutyrate are the three main ketone bodies examined, indicative of diabetic ketoacidosis. Nitroprusside is used to detect them.
- Serum lactate level –
If the lactate levels exceed 4-5 mEq/L, it indicates acidemia.
- Salicylate and iron levels –
Iron toxicity is related to lactic acidosis. A level exceeding 300 mg/dl is toxic. Salicylate levels in plasma beyond 40-50 mg/dl is harmful.
- Plasma renin activity
-
Trans-tubular potassium gradient
-
Ammonium chloride loading test
-
Imaging studies and Electrocardiography –
X-Rays of the abdominal area (ureters, kidney, bladder), CT scan of kidneys or ultrasound are helpful in detecting kidney stones. ECG may help to detect changes in the heart and circulatory system as a result of hyperkalemia.
Treatment of acidosis :
Management of acidosis is aimed at increasing the pH levels to 7.20. This is possible by treating the cause of the condition either directly or indirectly.
For respiratory acidosis, treatment employed is –
-
Bronchodilators are used to reverse some types of airway obstructions
-
Oxygen supply should be adequate
-
Non-invasive positive pressure ventilation
-
Acetazolamide (for bicarbonate excretion) can be used, but with caution
-
Drug antagonists such as naloxone (for opioid overdose) in cases of poisoning
For metabolic acidosis –
-
Bicarbonate infusions
-
ACE inhibitors are used to lower the levels of potassium (type 4 tubular renal acidosis)
-
Insulin is given intravenously for diabetic ketoacidosis, starvation.
-
Restoration of tissue oxygen in lactic acidosis
-
Drugs to counteract in cases of methanol poisoning or salicylate poisoning
What is alkalosis?
It is an excessively alkaline condition of the body, where the pH level crosses 7.45. Here the
decreased H+ ions concentration is decreased resulting in an increased bicarbonate concentration.
Classification :
-
Respiratory alkalosis
-
Metabolic alkalosis
What is respiratory alkalosis?
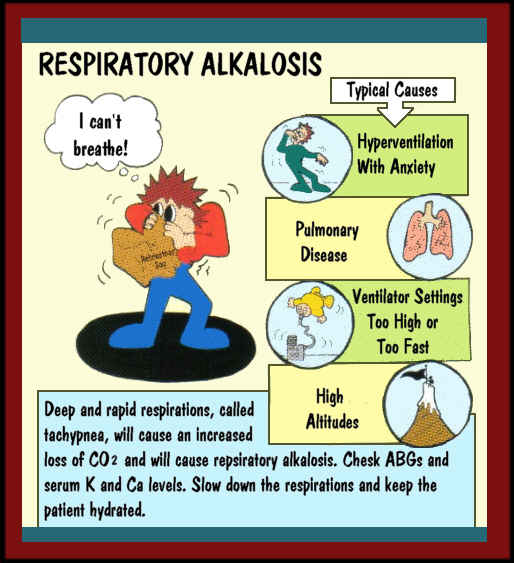
It is a condition where the blood pH levels go above the normal range (above 7.45) due to increase in respiration. The blood carbon dioxide levels dip down, causing alkalemia (blood pH above 7.45).
Respiratory alkalosis can be acute (has occurred in a short span of time) or chronic (happening over a long period of time).
Causes :
Any reason which makes a person hyperventilate (increased rate of breathing) will bring about respiratory alkalosis. Hyperventilation will cause more expulsion of carbon dioxide from the body, hence disturbing its equilibrium in the circulation. The body in its attempt to compensate will activate more of carbonic anhydrase enzyme to produce carbonic acid (H2CO3), a reversible intermediate which breaks down later to form CO2 and H2O. The extra H+ ions are utilised in this process which decreases overall free H+ ions. This decrease will make the blood more alkaline.
The reasons for respiratory alkalosis include :
-
Central Nervous System causes – pain, anxiety, hyperventilation syndrome, psychosis, fever, trauma, cerebrovascular accident, etc.
-
Hypoxia (low oxygen saturation in blood) related causes – high altitude, right to left shunts (heart failure)
-
Hormonal (endocrine) causes – pregnancy, hyperthyroidism
-
Drug-related – progesterone, salicylates, nicotine, methylxanthine toxicity
-
Pulmonary causes – emphysema, bronchitis, pulmonary edema, aspiration, etc.
-
Miscellaneous – sepsis, severe liver failure, anemia, mechanical ventilation
Check the signs :
-
The person may have fast heart beats (tachycardia) and fast, shallow breathing (tachypnea).
-
Peculiar rise and fall in chest movements
-
Cyanosis and other associated symptoms of respiratory disease such as crepitations (crackling sound), wheezing are seen
-
If the cause is CNS (nervous system) related, the person can have depressed levels of consciousness.
-
Cardiac disturbances are possible
Metabolic Alkalosis :
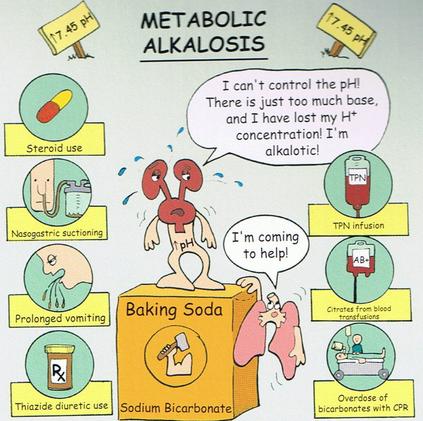
Contrary to metabolic acidosis, metabolic alkalosis represents a condition where the tissue pH goes beyond the upper limit of our pH range (>7.45). It is marked by decreased hydrogen ions concentration and an increase in the bicarbonate content (>35mEq/L).
The gastro-intestinal tract and kidneys are primarily involved in metabolic alkalosis. There are four mechanisms that contribute to metabolic alkalosis :
Causes :
The causes can be divided into two variants based on urine chloride levels –
-
Chloride responsive (urine chloride <10mEq/L)
-
Chloride resistant (urine chloride >20mEq/L)
Chloride responsive :
-
Loss of hydrogen ions –
When a person vomits, all the gastric secretions (HCl) are lost. For every hydrogen ion lost, there is a gain of bicarbonate ion. Excess of aldosterone hormone also helps in removal of hydrogen ions, which again makes everything more alkaline.
-
Congenital chloride diarrhea
-
Cystic fibrosis
-
Contraction alkalosis –
Any chloride rich fluid in extracellular compartment, as in thiazide or loop diuretics will decrease the total fluid levels of the body and increase bicarbonate concentration. This is because, the volume of body fluids has ‘contracted’ or shrunk.
Chloride resistant :
-
Retention of bicarbonate
-
Shift of hydrogen into intracellular space – seen in hypokalemia (low serum potassium levels). The potassium goes out of the cells and as compensation the hydrogen ions move in to maintain equilibrium, but end up increasing the pH.
-
Alkali administration –
Sodium bicarbonate when given from outside beyond the filtration capacity can induce alkalosis. Impaired kidney function also contributes to alkalosis because of its poor capacity to metabolise bicarbonate.
-
Hyperaldosteronism –
Excess of aldosterone hormone (Conn‘s syndrome) increases the sodium hydrogen exchange in the kidney, which makes for quicker extraction of hydrogen from the kidney.
-
Barter Syndrome, Gitelman syndrome
-
Aminoglycoside toxicity which promotes hypokalemia
Diagnosis of alkalosis :
-
Imaging studies –
Chest radiography is done to ascertain whether the cause is a pulmonary disorder or not. Pneumonia, pneumothorax, etc. are detected on chest X-rays. CT scan is used if chest X-rays are inconclusive and a more specific route is needed. Pulmonary embolism can be detected on a spiral CT.
Renal doppler ultrasound, renal angiography can detect renal artery stenosis (narrowing). CT scan of adrenal glands helps in ruling out hyperaldosteronism and Cushing’s syndrome.
Brain MRI scan can give a clue to cerebrovascular accident, brain tumors or trauma to the head.
-
Serum electrolytes –
Levels of sodium, potassium and phosphates are screened for any fluctuation in their levels. Bicarbonate is excreted by kidneys in compensation to respiratory alkalosis. A Davenport diagram helps in these cases.
-
Serum Anion Gap –
With this it is possible to differentiate between actual metabolic alkalosis and metabolic compensation for respiratory acidosis. Serum anion gap is elevated more in metabolic acidosis because of increased negative charge between albumin and more production of lactate.
-
Complete blood cell count –
If the white blood cells are higher than normal, sepsis is indicated
-
Thyroid testing – for hyperthyroidism
-
Liver function tests – indicate hepatic failure
-
Drug screens to rule out poisoning
-
Diuretic screens for patients with unexplained hypokalemia
-
Plasma renin and aldosterone levels for detecting disorders of adrenal gland e.g. Cushing’s syndrome
Alkalosis – Management :
Respiratory alkalosis is usually not a life threatening disease, and control of the causative factor relieves the person of the disease. Treatment approach –
-
Always monitor critically ill patients like those on mechanical ventilators. Their medication (sedatives, painkillers, etc.) should not be inadequate which would otherwise increase the risk of alkalosis.
-
For people who are hyperventilating, reassure them, try to relieve them of their stress. Ask them to breathe in a paper bag. This helps in reuptake of some exhaled carbon dioxide.
-
Beta adrenergic blockers are given to control hyperadrenergic state which causes hyperventilation.
-
After the cause of alkalosis has been estimated, it‘s best to consult a specialist for appropriate treatment of the underlying cause.
The principle behind treating metabolic alkalosis is first to treat the cause and then manage the factors that maintain the cause –
-
IV saline, chloride or potassium can be given to stop renal excretion of bicarbonate.
-
Acetazolamide acts in alkalosis almost immediately, but should be used with caution.
-
HCl infusions help in correcting chloride deficiency.
Compensatory changes in acidosis and alkalosis :
| Acid Base Disorder | Initial Chemical Change | Compensatory Response |
| Respiratory Acidosis | ↑ PCO2 | ↑HCO3- |
| Respiratory Alkalosis | ↓ PCO2 | ↓ HCO3- |
| Metabolic Acidosis | ↓ HCO3- | ↓ PCO2 |
| Metabolic Alkalosis | ↑ HCO3- | ↑ PCO2 |
Who is at the risk of Acidosis and Alkalosis?
Certain risk groups for acidosis include –
-
People consuming a high-fat low carb diet
-
Obese people with a very high Body Mass Index
-
Dehydration – less water intake beyond tolerable limits
-
People with a history of diabetes
-
People who tend to over consume drugs, which in turn puts a pressure on the liver and kidneys
People at risk for alkalosis –
-
Those who have respiratory disorders
-
People who consume excess of antacids
-
Dehydration
-
Risk of congenital disorders
Our body tries to maintain a constant state of equilibrium in many respects. Apart from a few causes, acid base irregularities and their consequences can be easily avoided at home. This begins with leading a healthy lifestyle and getting regularly checked by your doctor. As they say, ‘eternal vigilance is the cost of freedom (here, from diseases).’